Ozempic vs. Bariatric Surgery: Which Offers a Safer, Permanent Path to Health

As a board-certified Bariatric Surgeon, my commitment is to provide my patients with the safest, most effective, and most sustainable long-term solution for treating obesity and associated metabolic diseases. In the current medical landscape, many individuals are turning to Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 RAs) like semaglutide (Ozempic, Wegovy), viewing them as a simple, non-surgical “magic bullet.”1 However, the growing body of real-world evidence and clinical data reveals that these medications carry a spectrum of significant risks—from debilitating gastrointestinal issues to emerging, serious long-term complications—all coupled with an expectation of lifelong dependency and prohibitive cost.
This comprehensive analysis details the established and potential risks of semaglutide use, offering a vital contrast to the predictable, definitive, and superior outcomes achievable through established surgical procedures such as Gastric Sleeve, Gastric Bypass, and SADI-S.
The Cost of Dependence: Semaglutide’s Long-Term Financial and Physical Burden
The primary difference between pharmaceutical and surgical treatments for obesity lies in their fundamental approach: management versus definitive intervention. Semaglutide, while effective in the short term, treats obesity as a chronic condition requiring indefinite, weekly administration.
A. The Predictable Return of Disease: Weight Regain Upon Discontinuation
Clinical trials and real-world usage consistently confirm a major limitation of semaglutide: the inevitability of significant weight regain once the medication is stopped. The drug functions by manipulating the body’s appetite and satiety hormones. When the weekly injection is discontinued, these powerful hormonal and metabolic safeguards against weight loss reassert themselves.
Clinical Evidence of Regain: In studies like the STEP 1 trial, participants who achieved significant weight loss on semaglutide regained approximately two-thirds of that lost weight within one year of stopping the medication.
The Biological Mechanism: The drug suppresses “food noise” and reduces appetite. Once stopped, the returning hunger cues and the body’s naturally slowed metabolism post-weight loss (a defense mechanism against starvation) conspire to quickly reverse the patient’s progress. This creates a cycle of dependency, forcing patients to remain on the medication—and endure its risks—for life simply to maintain results.
B. The Prohibitive and Ongoing Financial Cost
For patients without robust insurance coverage, the financial commitment to semaglutide is staggering, accumulating into a significant debt over a lifetime.
Accumulated Costs: The annual cost for brand-name GLP-1 RAs can range from $$12,000 to over $\$16,000$ per year without insurance, or roughly $\$1,000$ to over $\$1,300$ per month. Over a typical twenty-year span of adult life, this financial burden can easily exceed $$250,000 for just one medication, not accounting for price increases or the cost of treating associated side effects.
The Contrast with Surgery: Bariatric procedures like the Gastric Sleeve or Gastric Bypass offer a definitive, one-time investment that is exceptionally cost-effective, particularly when accessed through specialist medical tourism centers like ours in Tijuana, Mexico. The initial, all-inclusive cost of surgery quickly pays for itself by eliminating lifelong drug expenses and reducing the need for costly medications for co-morbidities (like diabetes and hypertension).
II. Emerging and Serious Complications: The Spectrum of Semaglutide Side Effects
While the medication is lauded for weight loss, the data shows an increasing number of both common and serious potential side effects that pose a continuous threat throughout the period of use.
A. The Chronic Gastrointestinal Struggle
The most frequently reported issues are not merely minor nuisances; they are debilitating gastrointestinal disturbances that often lead to non-adherence and discontinuation. Real-world studies show that up to 20%-50% of patients discontinue the drug within the first year, primarily due to these GI issues.
Common Symptoms: Nausea (the most prevalent), vomiting, diarrhea, constipation, and abdominal pain are frequent, especially during dose escalation.
Severe Stomach Problems (Gastroparesis): Semaglutide functions by slowing gastric emptying. In severe cases, this can lead to gastroparesis (stomach paralysis) and, rarely, intestinal blockage (ileus). This condition is characterized by persistent severe nausea, vomiting, and debilitating abdominal cramping. While the aim is to reduce appetite, a severely slowed stomach can become a chronic, painful condition.
C. The Medullary Thyroid Carcinoma (MTC) Boxed Warning
A critical and alarming risk is the FDA Boxed Warning carried by semaglutide regarding the potential for thyroid C-cell tumors, including medullary thyroid carcinoma (MTC).
Rodent Studies: This warning is based on animal studies, where the medication caused thyroid tumors.
Human Risk: While it is not yet known if this risk translates directly to humans, the possibility is serious enough to warrant a mandatory contraindication. Patients with a personal or family history of MTC or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) must not use the drug. Patients are advised to watch for signs like a lump or swelling in the neck, hoarseness, or trouble swallowing. This represents a long-term risk that simply does not exist after a definitive bariatric procedure.
III. The Emerging Threat to Vision: Ocular and Neuro-Ophthalmic Complications
Recent observational studies have raised serious concerns regarding semaglutide’s potential association with grave eye conditions, including those that can cause permanent vision loss. While the absolute risk may be low, the consequences are devastating, and the association demands attention.
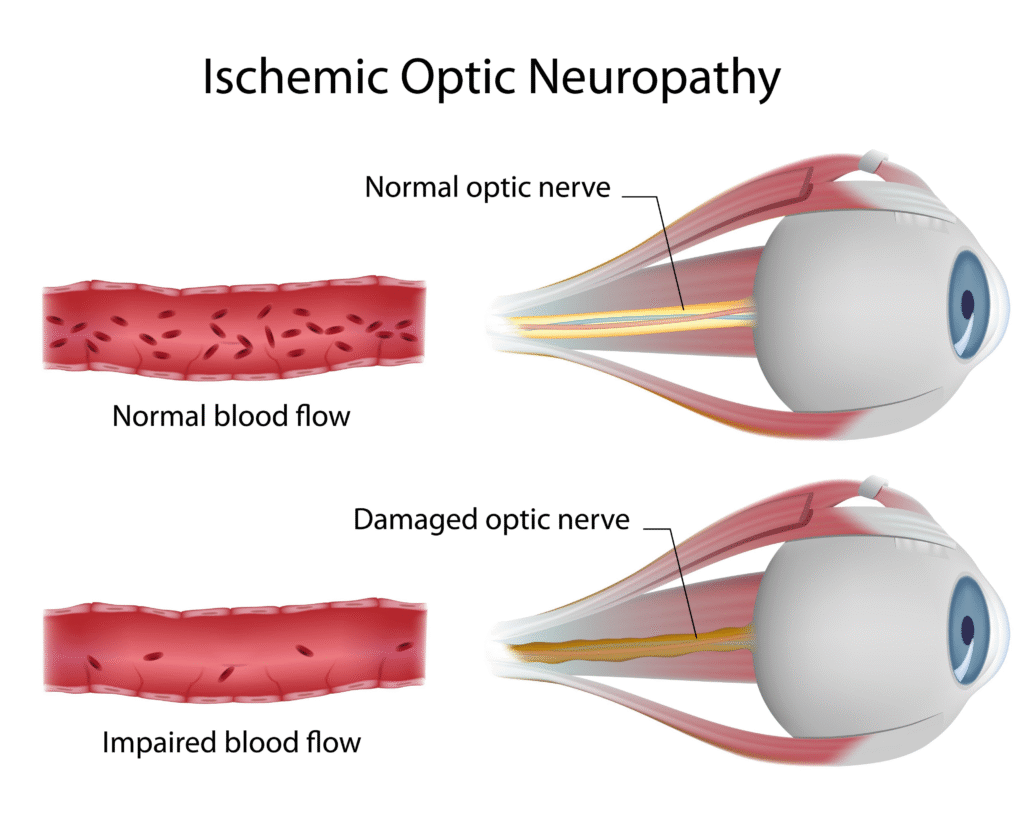
A. Nonarteritic Anterior Ischemic Optic Neuropathy (NAION)
A study published in JAMA Ophthalmology investigated the possibility that semaglutide is associated with Nonarteritic Anterior Ischemic Optic Neuropathy (NAION). This condition, sometimes morbidly nicknamed “Ozempic blindness,” is caused by a blockage of blood flow to the optic nerve, leading to sudden, painless, and often permanent vision loss in one eye.
Key Finding: The study found a significantly higher risk of NAION for patients receiving semaglutide compared to those on non-GLP-1 RA medications.
In the type 2 diabetes (T2D) group, the hazard ratio (HR) for NAION was 4.28 (95% CI, 1.62-11.29) for semaglutide users.
In the overweight/obese group, the HR for NAION was even higher at 7.64 (95% CI, 2.21-26.36).
Conclusion: The findings suggest a clear association between semaglutide and NAION. While formal causality still requires further study, the significant increased risk is a major concern for any patient considering lifelong therapy.
B. Worsening of Diabetic Retinopathy
For patients who already have Type 2 Diabetes, semaglutide can cause complications due to the rapid improvement in blood sugar control. This rapid change can temporarily worsen pre-existing diabetic retinopathy (damage to blood vessels in the eye), potentially leading to retinal bleeding, swelling, or requiring laser treatment. Regular eye exams are therefore critically important for diabetic patients on these drugs, adding another layer of cost and monitoring.
IV. The Definitive Metabolic Solution: Bariatric Surgery
As the data on GLP-1 RAs matures, the evidence increasingly solidifies the position of bariatric and metabolic surgery—specifically Gastric Sleeve, Gastric Bypass, and SADI-S—as the most effective, safest, and most cost-effective long-term solution. These procedures are not merely for “weight loss”; they are powerful metabolic interventions.
A. Superior Long-Term Results and Sustained Weight Loss
Unlike medications that require continuous use to prevent weight regain, bariatric surgery provides a physical and hormonal reset that is permanent.
Mechanism of Action: Procedures like the Gastric Sleeve (Sleeve Gastrectomy) and Gastric Bypass work by dramatically reducing stomach size and fundamentally altering gut hormone signaling in a way that is more robust and lasting than medication. SADI-S (Single Anastomosis Duodeno-Ileal Bypass with Sleeve) is an advanced procedure that offers even greater metabolic and long-term weight loss benefits.
Sustainable Results: Patients achieve a definitive weight loss result, with studies showing sustained weight loss for a decade or more, leading to a far lower risk of significant weight regain compared to medication discontinuation.
B. Definitive Resolution of Associated Illnesses
The fundamental benefit of these procedures is their profound metabolic effect. They are not drugs designed merely to control insulin; they are treatments that can lead to the remission of the disease itself.
Type 2 Diabetes Remission: Bariatric surgery—particularly the Gastric Bypass and SADI-S—is recognized as the single most effective treatment for Type 2 Diabetes, with success rates for remission (no longer requiring medication) far surpassing what is achievable with lifelong drug therapy.
Control of Co-morbidities: Surgery leads to the resolution or significant improvement of hypertension, high cholesterol, sleep apnea, and fatty liver disease. This eliminates the need for multiple lifelong medications, translating directly to profound health and financial benefits.
C. Safety, Predictability, and Finality
The safety profile of modern bariatric surgery is excellent, comparable to common procedures like gallbladder removal.
Acute vs. Chronic Risk: Surgery carries an acute, temporary risk during the perioperative period (the first few weeks of recovery), after which the risk drops significantly. In stark contrast, semaglutide carries chronic, lifelong risks that persist every day the patient is on the medication (Pancreatitis, Thyroid Tumor risk, NAION risk, etc.).
Freedom from Dependency: Patients gain freedom from weekly injections, unpredictable side effects, and the crushing financial weight of lifelong drug dependency. They transition from managing a disease with daily injections to being a post-surgical patient focused on a new, healthy life.
Conclusion
For individuals struggling with obesity and its associated diseases, the choice is clear: manage the disease indefinitely with emerging risks and recurring high costs, or intervene definitively with a proven, safe, and permanent metabolic solution.
The body of evidence confirms that while semaglutide offers a form of weight control, it locks patients into a relationship with a drug that carries a continuous, and in some cases, serious, risk profile (including GI distress, pancreatitis, gallbladder issues, the FDA’s MTC warning, and the emerging risk of vision loss like NAION).
As your Bariatric Surgeon, I advocate for the definitive path. Gastric Sleeve, Gastric Bypass, and SADI-S offer a proven, single-step intervention that provides:
Superior, Sustainable Weight Loss.
High Rates of Type 2 Diabetes Remission and Resolution of Co-morbidities.
Freedom from Drug Dependency and its Associated Chronic Health Risks.
Exceptional Long-Term Cost-Effectiveness.
We invite you to stop chasing temporary, risky management plans. Choose the peace of mind and definitive health resolution that comes with an established metabolic procedure. Your life-changing journey begins with a choice for permanence, safety, and superior health.
Contact our office in Tijuana, Mexico, today for a confidential consultation to explore which life-changing metabolic procedure is right for you.

